M.Koushiki
R.n 79 3rd sem
Under the guidance of Dr. Sai Vittal sir (Intern)
This is an online E log book to discuss our patient's deidentified health data shared after taking his/her/guardian's signed in formed consent.Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence-based inputs .
I have been given this case to solve in an attempt to understand the topic of patient clinical data analysis to develop my competency in reading and comprehending clinical data including, history, clinical findings, investigations, and come up with a diagnosis and treatment plan.
CASE SCENARIO:
A 48 yr old male patient came to the ward on 6 July 2021 with chief complaints of distended abdomen since 5 days, and pedal edema for 1 month and shortness of breath since 2 days and loose stools on the day of admission.
HISTORY OF PRESENTING ILLNESS
Patient was apparently asymptomatic till 4 months back ,then he had abdominal distension and diagnosed with Decompensated Liver Cirrhosis
c/o shortness of breath (grade II - grade III)
c/o B/L pedal edema (upto knee)- pitting type ,loose stools (watery consistency)- 2 to 3 episodes
No c/o othopnoea,PND ,palpitations, sweating.
HISTORY OF PAST ILLNESS
K/C/O DM since 1 yr
TREATMENT HISTORY
On medication for DM
Tab. GLIMI - M1
PERSONAL HISTORY
Married
Occupation: Daily wage labourer
Diet: Mixed , Non vegetarian
Appetite: Normal
Bowels: Regular
Known Allergies: No
Addictions: alcoholic ( since 12yr 90ml for 2 to 3 Days) and regular intake since 10 yr( 180ml daily )
Tobacco chewing since 20 yrs
FAMILY HISTORY
No H/O similar complaints in the family
GENERAL EXAMINATION
Patient is conscious and coherent
Moderate built and moderately nourished
Well oriented to time, place and person.
No pallor
Icterus present
No cyanosis
No clubbing
No lymphadenopathy
Oedema of feet -present ++
No malnutrition
No dehydration
VITALS:
Temperature-afebrile
Pulse rate- 112/min
Respiratory rate- 20/min
BP- 130/80mmHg
SPO2 - 91%
GRBS- 114mg%
SYSTEMIC EXAMINATION
CARDIOVASCULAR SYSTEM
Thrills: No
Cardiac sounds: S1 , S2
Cardiac murmurs: No
RESPIRATORY SYSTEM
Dyspnoea:present ( grade II- grade III)
Wheeze: No
Position of trachea: Central
Breath sounds: Vesicular
Adventitious sounds : No
ABDOMEN
Shape - Scaphoid
No tenderness, palpable mass,
Fluid - present
No bruits
CENTRAL NERVOUS SYSTEM
Level of consciousness - conscious
Speech - Normal
No signs of meningeal irritation
Cranial nerves - Normal
No motor or sensory deficit
Reflexes
Biceps Triceps Supinator Knee Ankle
Right 2+ 2+ 2+ 2+ 2+
Left 2+ 2+ 2+ 2+ 2+
PROVISIONAL DIAGNOSIS:
Decompensated Liver Cirrhosis k/c/o dm II
INVESTIGATIONS
Hemogram, LFT, RFT, Chest Xray,PT, ECG ,APTT,Ascitic fluid analysis,USG Abdomen
HAEMOGRAM
LIVER FUNCTION TEST
RENAL FUNCTION TEST
PROTHROMBIN TIME
SAAG
APTT
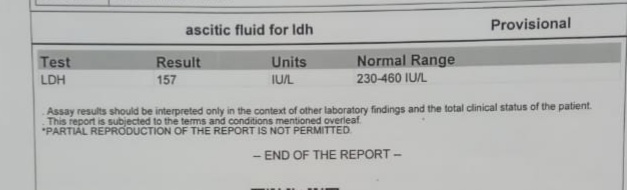
ASCITIC LDH
ASCITIC FLUID AMYLASE
ASCITIC FLUED PROTEIN SUGAR
CHEST XRAY




ECG
Icterus
Pedal oedema
DIAGNOSIS:
DECOMPENSATED LIVER CIRRHOSIS with
TYPE II DIABETES MELLITUS
Update on Day 07/07
TREATMEN GIVEN
1. Salt Restriction <2.4 g/day
2. Fluid Restriction <1 lit/day
3. Syrup Lactulose 10ml/PO/TID
4. INJ. Thiamine 1 ampule 500ml NS/IV/OD @2pm
5. INJ. Optineuron 1ampule in 500ml NS/IV/OD
6. INJ. Vit K 10mg IV/OD (over 30 min)
7. TAB. LASILACTONE (20/50mg) PO/OD
8. 3 eggs whites/day
9. TAB. SPOROLAC -D PO/STAT
10. ORS SACHET IN 1lit of water whole day
11. TAB. UDILIV 300mg PO/BD
12. TAB. OXAZEPAM 15mg
x - 2 - 2 for 2 days
13.TAB. PREGABA 75mg
x - x - 1
14. NICOTEX GUMS 2mg
1 - 1 - 1
15. Protein powder 1 Tbsp in 1 glass of milk PO/OD
16. BP/PR/Temp SPO2 Monitoring 4th hourly
17. Daily weight and Abdominal girth
monitoring
Update on DAY 08/07
DIAGNOSED DECOMPENSATED LIVER CIRRHOSIS with TYPE II DIABETES MELLITUS
with SPONTANEOUS BACTERIAL PERITONITIS with GRADE I HEPATIC ENCEPHALOPATHY
Abdomen distended non tender
Abdominal girth 104 cm wgt 68kg
GRBS 160%
TREATMENT GIVEN
1. INJ. THIAMINE 1 amp in 100 ml NS IV/OD @2pm
2. INJ. OPTINEURON 1amp in 500ml NS IV/OD
3. INJ. VIT K 100mg IV/OD (over 30min )
1 - x - x
4. TAB. LASILACTONE (20/50mg) PO/OD
5.TAB SPOROLAC -D PO/STAT
6. TAB. OXAZEPAM 15 mg
x - 2 - 2 X2days
7. TAB. PREGABA 75mg
x - x - 1
8. SYP LACTULOSE 10ml PO/TID ( to maintain 2 episodes of losse stools)
9. ORS SACHET In 1lit of water whole day
10.TAB. UDILIV 300mg PO/BD
11. NICOTEX GUMS 2mg
1 - 1 - 1 SOS
12.Salt Restriction <2.4 g/day
13.Fluid Restriction <1 lit/day
14.Protein powder 1 Tbsp in 1 glass of milk PO/OD
15. BP/PR/Temp SPO2 Monitoring 4th hourly
16. 3 eggs whites/day
17. INJ. CEFOTAXIME IV/TID
18. INJ. LASIX 4mg IV/BD
19. INJ. PATOP IV /OD
20. GRBS 6th hourly
21. TAB. RIFAGUT 550mg PO/BD
22. TAB. PCM 500mg (dont exceed 2mg/day)
Runyon's criteria:
Protein <1
glucose <50mg/dl
LDH more than upperlimit for serum
LDH>240U/I
Child pugh score : 12 points class C 82% mortality
Meld score: 10 points 6% estimated mortality
Complete blood picture ( 08/07)
Liver function test ( 09/07)
Update on Day 09/07
C/O pain in hypochondrial region
Abdomen Distension present abdominal girth 106cm weight 70kg
Tenderness in left hypochondrium
GRBS 142mg%
Stools passed 2 times
TREATMENT GIVEN :
1. INJ. CEFOTAXIME 2gm IV/TID
2. INJ. THIAMINE 1 amp in 100 ml NS IV/OD @2pm
3. INJ. VIT K 100mg IV/OD (over 30min )
4.INJ. PATOP 40mg IV /OD
5. Salt Restriction <2.4 g/day
6.Fluid Restriction <1 lit/day
7.TAB. LASILACTONE (20/50mg) PO/OD
8.TAB. RIFAGUT 550mg PO/BD
9. SYP LACTULOSE 10ml PO/TID ( to maintain 2 episodes of losse stools)
10. TAB GLIMI - M2 PO/OD
11. PROTEIN POWDER 1 TBSP in 1 GLASS OF MILK PO/BD
12. INJ LASIX 40mg TID ( if SBP > or = 110mmHg)
13. TAB UDILIV 300mg PO/BD
14. 3Eegg whites/day
15. BP/PR/TEMP/SPO2 4th hourly
16. GRBS 6th hourly
17. TEMP CHARTING
Update on Day 10/07
Decompensated Liver disease (Cirrhosis) with spontaneous bacterial peritonitis with fracture of left radial styloid process with k/c/o DM II
c/o abdominal distension is persistent
Fever subsided sob reduced
Abdominal girth 104 cm weight 68kg
TREATMENT GIVEN:
1.INJ.PANTOP 40mg IV/OD
2. INJ. CEFOTAXIME 2mg IV/TID
3. Salt Restriction <2.4dm/day
4. Fluid Restriction <1.5lit/day
5. INJ. LASIX 40mg
6. TAB ALDACTONE 50mg PO/OD
7. TAB. UDILIV 300mg PO/BD
8. TAB. RIFAGUT 550mg PO/BD
9. 2 egg whites /day.
10. 2 tbsp of protein-x powder in 1 glass milk PO/TID
11. GRBS 6th hourly per meal
12. Strict I/O charting
13. BP/PR/TEMP charting hourly
14. TAB. THIAMINE 100mg PO/OD
15. INJ. HAL s/o acct to sliding scale
8am - 2pm - 8pm
DISCHARGE SUMMARY
Date: 11/07/2021
Ward: General medicine
Name of treating faculty:
Dr. Rakesh biswas ( hod )
Dr. Hareen ( sr )
Dr. Rashmitha ( pg y2 )
Dr. Divya ( pg y2 )
Dr. Nikitha ( pg y2 )
Dr. Manasa ( pg y1 )
Dr. Sai Vittal ( Intern )
Dr. Rishik ( Intern )
Dr. Roopa ( Intern )
Dr. Preethi ( Intern )
Dr. Deekshitha ( Intern )
DIAGNOSIS :
DECOMPENSATED LIVER DISEASE (CIRRHOSIS) with
SPONTANEOUS BACTERIAL PERITONITIS
with
HEPATIC ENCEPHALOPATHY grade I
with
radial styloid fracture with k/c/o DM TYPE II
CASE HISTORY AND CLINICAL FINDINGS
Patient was apparently asymptomatic till 4 months back ,then he had abdominal distension and diagnosed with Decompensated Liver Cirrhosis
c/o shortness of breath (grade II - grade III)
c/o B/L pedal edema (upto knee)- pitting type ,loose stools (watery consistency)- 2 to 3 episodes
No c/o othopnoea,PND ,palpitations, sweating.
PAST HISTORY
K/C/O DM since 1 yr
TREATMENT HISTORY
On medication for DM
Tab. GLIMI - M1
PERSONAL HISTORY
Married
Occupation: Daily wage labourer
Diet: Mixed , Non vegetarian
Appetite: Normal
Bowels: Regular
Known Allergies: No
Addictions: alcoholic ( since 12yr 90ml for 2 to 3 Days) and regular intake since 10 yr( 180ml daily )
Tobacco chewing since 20 yrs
FAMILY HISTORY
No H/O similar complaints in the family
GENERAL EXAMINATION
Patient is conscious and coherent
Moderate built and moderately nourished
Well oriented to time, place and person.
No pallor
Icterus present
No cyanosis
No clubbing
No lymphadenopathy
Oedema of feet -present ++
No malnutrition
No dehydration
VITALS:
Temperature-afebrile
Pulse rate- 112/min
Respiratory rate- 20/min
BP- 130/80mmHg
SPO2 - 91%
GRBS- 114mg%
SYSTEMIC EXAMINATION
CARDIOVASCULAR SYSTEM
Thrills: No
Cardiac sounds: S1 , S2
Cardiac murmurs: No
RESPIRATORY SYSTEM
Dyspnoea:present ( grade II- grade III)
Wheeze: No
Position of trachea: Central
Breath sounds: Vesicular
Adventitious sounds : No
ABDOMEN
Shape - Scaphoid
No tenderness, palpable mass,
Fluid - present
No bruits
CENTRAL NERVOUS SYSTEM
Level of consciousness - conscious
Speech - Normal
No signs of meningeal irritation
Cranial nerves - Normal
No motor or sensory deficit
Reflexes
Biceps Triceps Supinator Knee Ankle
Right 2+ 2+ 2+ 2+ 2+
Left 2+ 2+ 2+ 2+ 2+
INVESTIGATIONS DONE
Hemogram, LFT, RFT, Chest Xray,PT, ECG ,APTT,Ascitic fluid analysis,USG Abdomen
TREATMENT GIVEN
On07/07
1. Salt Restriction <2.4 g/day
2. Fluid Restriction <1 lit/day
3. Syrup Lactulose 10ml/PO/TID
4. INJ. Thiamine 1 ampule 500ml NS/IV/OD @2pm
5. INJ. Optineuron 1ampule in 500ml NS/IV/OD
6. INJ. Vit K 10mg IV/OD (over 30 min)
7. TAB. LASILACTONE (20/50mg) PO/OD
8. 3 eggs whites/day
9. TAB. SPOROLAC -D PO/STAT
10. ORS SACHET IN 1lit of water whole day
11. TAB. UDILIV 300mg PO/BD
12. TAB. OXAZEPAM 15mg
x - 2 - 2 for 2 days
13.TAB. PREGABA 75mg
x - x - 1
14. NICOTEX GUMS 2mg
1 - 1 - 1
15. Protein powder 1 Tbsp in 1 glass of milk PO/OD
16. BP/PR/Temp SPO2 Monitoring 4th hourly
17. Daily weight and Abdominal girth
monitoring
Day
On08/07
Same as the previous day inaddition
INJ. CEFOTAXIME IV/TID
TAB. RIFAGUT 550mg PO/BD
TAB. PCM 500mg (dont exceed 2mg/day)
On 09/08
1. INJ. CEFOTAXIME 2gm IV/TID
2. INJ. THIAMINE 1 amp in 100 ml NS IV/OD @2pm
3. INJ. VIT K 100mg IV/OD (over 30min )
4.INJ. PATOP 40mg IV /OD
5. Salt Restriction <2.4 g/day
6.Fluid Restriction <1 lit/day
7.TAB. LASILACTONE (20/50mg) PO/OD
8.TAB. RIFAGUT 550mg PO/BD
9. SYP LACTULOSE 10ml PO/TID ( to maintain 2 episodes of losse stools)
10. TAB GLIMI - M2 PO/OD
11. PROTEIN POWDER 1 TBSP in 1 GLASS OF MILK PO/BD
12. INJ LASIX 40mg TID ( if SBP > or = 110mmHg)
13. TAB UDILIV 300mg PO/BD
14. 3Eegg whites/day
15. BP/PR/TEMP/SPO2 4th hourly
16. GRBS 6th hourly
17. TEMP CHARTING
On 10/07
1.INJ.PANTOP 40mg IV/OD
2. INJ. CEFOTAXIME 2mg IV/TID
3. Salt Restriction <2.4dm/day
4. Fluid Restriction <1.5lit/day
5. INJ. LASIX 40mg
6. TAB ALDACTONE 50mg PO/OD
7. TAB. UDILIV 300mg PO/BD
8. TAB. RIFAGUT 550mg PO/BD
9. 2 egg whites /day.
10. 2 tbsp of protein-x powder in 1 glass milk PO/TID
11. GRBS 6th hourly per meal
12. Strict I/O charting
13. BP/PR/TEMP charting hourly
14. TAB. THIAMINE 100mg PO/OD
15. INJ. HAL s/o acct to sliding scale
8am - 2pm - 8pm
ADVICE AT DISCHARGE:
•Salt restriction 2.4 gm/day
•Fluid restriction 1.5L/day
•Tab cefatoxime 200 mg PO/BD for 4 days
•Tab lasix 40 mg PO/BD 8am --4pm
•Tab aldactone 50 mg PO/OD
•Tab Glimi M2 PO/OD
•Tab MVT PO/OD 2pm
•Tab limcee PO/OD
•Tab pcm 500 mg PO/SOS ( not more than 2gms/day)
•Protein powder-DM 2 tps in 1 glass of milk PO/TID







































Comments
Post a Comment